|
|
|
|
|
|
The Myths of Healing: A Summary of Research into Transpersonal Healing Experiences M. Allan Cooperstein Cooperstein, M. A. (1992). The myths of healing: A summary of research into transpersonal healing experience. Journal of the American Society for Psychical Research, 86, 99-133.
ABSTRACT
This descriptive study was undertaken to discover and describe the psychological
experiences
A sample of 10 books written by a variety of Transpersonal Healers was analyzed for content,
and 10
Shamanism is discussed as a concept that most closely represents the findings of this research; transpersonal healing is proposed as a range of contemporary subtypes of "pure" shamanic practice. The core process--termed the "Shamanic Complex"--is described in terms of the methodologies used intentionally to activate an endogenous human potential. A taxonomic system is proposed for use in parapsychological research. Transpersonal healers are individuals who attempt to influence beneficially the physiology of living organisms through the use of culturally unorthodox noninstrumental methods, including (a) the laying on of hands; (b) wishing; (c) acting as a source or "channel" for the transfer of purported healing "energies;" (d) shamanic healing; (e) prayer healing; (f) "magnetic" healing; (g) mystical healing; (h) diagnosing ailments or prescribing remedies through divine (or "inner") guidance; (i) the mediumistic incorporation of "spirits" or discarnate entities for the communication of information relevant to healing; 0) possession by "spirit doctors," whether for actual surgical procedures (see Puharich's [19741 description of Arigo, a Brazilian healer) or mock surgery on the "auric" or "etheric body" (Chapman & Stemman, 1984); (k) mystical "attunement" or merging" with the healee and/or a divine source of healing power; and (1) shrine and "power spot" healing. Healers often claim in their writings that alterations in consciousness and beliefs in special powers, spiritual realities, "energies," or entities are the causal factors in the production of anomalous healing effects and other related parapsychological phenomena. Psychologists generally refer to consciousness as a construct or concept denoting the sum of the relationships between mental processes. Many healers, however, refer to consciousness not as an abstraction, but as a concrete, fundamental awareness that is a basic attribute of existence possessed by all living things. Thus, psychologists use the term abstractly to express a synthesis of mental processes, whereas healers use it literally, to refer to a property of life in terms connoting (a) extensiveness, (b) nonlocality, and (c) the capacity to perform work (e.g., effect changes or movements in physical objects, relay information, or produce healing effects). If healers' assertions are to be credited with accuracy when empirically investigating anomalous healing effects, however, it is necessary to examine and understand their alterations in consciousness-in the psychological sense-and to posit possible mechanisms and mediums through which nonphysical consciousness-in the healer's sense-may interact with the physical world. Anomalous healing/influencing effects have been studied under controlled experimental conditions for almost 30 years, beginning with Grad's pioneering studies (see Grad, Cadoret, & Paul, 1961; also see Solfvin's 1984 review of the literature). Although empirical investigations continue, the majority of studies primarily emphasize the presence or absence of an effect and the adequacy of research methodology and design in the validation and measurement of purported effects rather than exploring the means by which effects are produced. Rather than merely limiting research to the measurement of "treatment" effects followed by post hoc speculation about the means by which healers may have accomplished this end, descriptive information of the healers' experiences could delineate the psychological processes involved in transpersonal healing for future experimental and clinical investigations (see Neher, 1980, p. 293). Consequently, the principal goal of this research was to discover and describe the experiences of healers/influencers during healing attempts. A second goal called for the development of a taxonomic system capable of differentiating between varieties of healers/influencers; this system would be based upon differences in the psychological processes utilized by the healers rather than a continued reliance upon misleading labels derived from the speculations of healers or researchers. Further, it was hoped that information emerging from this research could stimulate the generation of hypotheses related to new or existing models of transpersonal healing (see Krippner & Villoldo, 1976) and parapsychological influencing (Stanford, 1977). In this paper I summarize my doctoral research, which was aimed at uncovering the psychological experiences of a sample of 20 transpersonal healers during healing attempts (see Cooperstein, 1990). Due to a lack of prior research and an absence of an appropriate research algorithm, I developed and applied an exploratory, multiphasic methodology designed to objectify healers' statements. Because of its unusual nature, each phase of the research process is described. An abstract of the descriptive information produced is provided. Based upon these data, a taxonomy of healers is presented. I conclude by discussing and comparing the shamanic experience, proposing that the varieties of transpersonal healing are contemporary adaptations of shamanism with possible endogenous roots.
RESEARCH METHOD Heuristic Research Given the uncertain and as yet undetermined nature of the transpersonal healing process itself, a flexible, evolving methodology was required in order to avoid superimposing a predetermined, rigid, or narrow research approach that could blunt the sensitivity of observations and jeopardize the exposure and exploration of unanticipated or unknown factors. Such factors, if brought to light, could lead to the generation of fruitful hypotheses and open new avenues of research. For this purpose heuristic inquiry was selected as the method of choice. Heuristic methodology offers the necessary flexibility without compromising the researcher's objectivity through commitment to a single theoretical perspective. This permitted necessary changes in research direction as dictated by the situation. Reliance solely upon empirical methods could have limited the flexibility, sensitivity, and scope of the dimensions needed to undertake a creative, yet disciplined, exploration of human capacities and meanings.
Research Assumptions An analysis of the literature in combination with the choice of methodology resulted in the following assumptions:
Sampling Data sources were selected as purposive samples. On the use of such samples, Chein (1981) states:
Similarly, Polkinghorne's (1983) views support the basic reasoning underlying the choice of nonprobabilistically-based sampling from the perspective of humanistically-oriented human science research:
In addition, nonprobabilistic sampling has the advantages of convenience and economy. Due to the exploratory nature of this descriptive study, generalizability is not of immediate concern.
PROCEDURE Phase 1: Preliminary Analysis A cross-sectional survey and analysis of some of the writings of transpersonal healers (suggested by researchers in the field) was performed (see Appendix 1). Experiences common among these healers were organized within conventional categories of experience: cognition, sensation, perception, attitudes, values, beliefs, etc. Due to the sometimes ineffable, transient, and/or nonordinary experiences encountered by transpersonal healers, the descriptive terms used were often found to be too vague and/or idiomatic to lend themselves easily to capture by orthodox psychological concepts and terminology. Further conceptual modification and refinement was required. Phase 2: Refinement of Items Seeking to increase objectivity among writers, a second, more intensive analysis was conducted in order to modify and refine the pool of experiential items; this was performed upon the (presumably) more unbiased written reports of three scholarly healer-researchers: Rebecca Beard (I 95 1), Delores Krieger (I 979), and Lawrence LeShan (I 975). The data of both analyses were then combined, and items were reorganized using Tart's (1975a) systems approach to consciousness in order to encompass ordinary and transpersonal experiences (see Tart, 1975b). Phase 3: Scoring Protocol Development: The Inventory of Transpersonal Healing Experience Individual spreadsheets were constructed for each experiential area, organized by headings, subheadings, and items. From this structure, a scoring tool in booklet form-the Inventory of Transpersonal Healing Experience (ITHE)-was developed for the systematic scoring of the experiential features encountered in texts and interviews (see Appendix 2). The ITHE was to be used in frequency analyses. This was supplemented by areas/items suggested by the work of Deikman (1972a, 1972b), Joy (1978), LeShan (1969, 1975), Osis, Bokert, and Carlson (1973), Pekala (1985), Pekala and Levine (1981-82), Pekala and Wenger (1983), Roberts (1981), and Tart (1975a). Scores were transferred from ITHE booklets to spreadsheets for computation. A 3-point coding system (2, 1, or 0) indicated the presence or absence of experiential features in texts. Statements clearly indicating the presence of a feature or process were coded 2; when context-sensitive inferential processes were used to determine the presence of a component for which no direct statement was presented, a I was assigned; no mention of an experiential area or item was scored 0. In unclear situations, conservative decisions were made to score items as 0. The same method was applied in analyzing interviews: Frequently experienced items were scored 2; less frequently experienced items received a 1; when interviewees reported uncommon and rare experiences, .5 was used. Items that were not part of the healer's experience or for which the healer/influencer expressed doubt that they had ever occurred were assigned 0. This system was chosen in order to extend the limits of a simple binary system, allowing for inclusion of less clearly stated inferential data while minimizing their impact on the whole through decreased weighting. Phase 4: Selection of Research Samples Books. A sample of 10 narrative and/or teaching texts was chosen that represented a cross-section of common types of transpersonal healing (see Table 1). Books were selected according to the following criteria:
Interview participants. Candidates meeting the standards for inclusion were suggested by investigators in the field of transpersonal healing. The sample was narrowed to 10, based upon the following criteria:
The sample of interviewees included 5 males and 5 females with a mean age of 53.9 years. All participants were first contacted by telephone and informed about (a) the identify of the researcher and his relationship to Saybrook Institute, (b) the nature of the research and its goal, (c) the anticipated length of the interview (approximately 2-3 hours), (d) the voluntary basis for participation and waiver of the right to anonymity, (e) the structure of the interview and safeguards in the event of fatigue, (f) the researcher's intent to tape-record the dialogue for purposes of scoring and content analysis, and (g) the freedom to withdraw at any point. Agreement was reached in all cases, and appointments were set for the interviews.
Phase 5: Analysis and Interviews Texts were analyzed page by page, comparing the healers' statements with ITHE areas/items and scoring them accordingly. At times, an author's statement might result in an inferentially-derived item score (i.e., 1). Inferentially-derived scores were considered tentative and could be altered to 2 or 0 if subsequent statements clarified the presence or absence of the feature or process. Semistructured interviews were then conducted, following the structure of the ITHE. Because of the geographical distribution of interviewees, telephone interviewing (and tape recording) was performed in all instances but one. In that case, the researcher met with the participant in her home but conducted the interview in a fashion similar to telephone interviews. One interviewee was not fluent in English. The interview was conducted through a Polish interpreter using a three-way conference line. Interviews were structured as follows:
Content analysis scores were transferred to spreadsheets. Interview tapes were replayed for ITHE scoring, and scores were transferred to spreadsheets. Descriptive data were analyzed, and response frequencies were calculated, incorporating three equal class intervals-High, Medium, and Low (McCall, 1986); these were presented in tabular form, grouping data within subareas. Finally, the contribution of each major experiential area to the overall healing experience was assessed by averaging healers' and influencers' rankings of experiential areas.
RESULTS Averages derived from the healers' rankings indicated that the main experiential components associated with the alterations in consciousness reported by transpersonal healers/influencers involve modifications in (a) sense of self (i.e., personal identity), (b) attention, and (c) cognitive processes, respectively (see Table 3). There follow example quotations extracted from interviewees' recordings that illustrate these experiential components. Italics have been inserted to emphasize important points. Healers apply a variety of approaches in realizing, or "making real," their intent to heal. These include (autosuggestive) verbal affirmations and the creative use of imagination (both as nonimaginal beliefs and mental imagery) to loosen and extend the conceptual boundaries and limits of physical reality.
The principal beliefs associated with transpersonal healing include those associated with (a) nonordinary energies, powers, and forces, (b) discarnate (spiritual and spiritistic) beings, and (c) parapsychological abilities that augmented the known range of human faculties. Although healers often resort to explaining their experiences in terms of their beliefs, these beliefs are used metaphorically as a means of interpreting and communicating experiences. For example:
Many healers believe that consciousness is a fundamental organismic awareness existing as an extended, nonlocal, distinguishable entity not limited to humans but possessed by all living (and possibly nonliving) things, which is thus capable of interacting with the physical world. Individual consciousness is believed to be limited by personal identity; they say that by setting this aside, it becomes possible to merge one's being, or consciousness, with that of another organism (or object) in order to acquire information and/or to influence the other. Healers report that personal control over cognitive processes is increased at "treatment" onset through the use of self-regulative, meditative techniques such as centering, meditative prayer, and healing meditations.
At first, healers note that their attention is concentrated effortfully by focusing upon a single (internal or external) aspect of experience while rejecting irrelevant sensory input.
According to the healers, eventually a shift in awareness occurs that is characterized by (a) decreased effort, (b) enhanced awareness of and sensitivity towards inner events and processes (although without the total exclusion of external reality), and (c) intense absorption within, or surrender to, the object of attention.
Although awareness of the general, external environment is reported to decrease, sensitivity (i.e., receptivity) ordinarily is experienced as increased towards a single aspect of the environment, namely the healee.
The healers indicate that motor activity is generally reduced at first, and alterations in meaning (or the interpretation of perceptions) commonly occur.
Although the majority of healers report having induced a nonordinary state of hypoarousal during which heart, pulse rate, body tonus, and respiration were decreased, the descriptions of two interviewees corresponded with the induction of a hyperaroused state. Both approaches appear to be used to destabilize the ordinary, or baseline, state of consciousness (see Tart, 1975a). In association with these changes in consciousness, a variety of nonordinary physical sensations may be experienced, including (a) quasi-energy feelings, (b) variations, (c) oscillations or rhythmic reverberations, and (d) thermal changes involving extraordinary warmth or coldness.
The healers reported their time sense as often altered. A sense of timelessness is most common, although other temporal distortions are also reported.
In comparison with normal mentation, thinking is experienced as more nonanalytical, noncritical, and expectant (i.e., in line with the healers' initial goalsetting). The healers claim that inner speech (i.e., discursive thought) usually decreases and may reach a point of "inner silence."
Healers describe an increased tolerance of ambiguity and decreased dualistic thinking. In addition, the healers claim that emotional responses are typically heightened during transpersonal healing. These are primarily positive emotions, although negative emotions are reported occasionally.
The above processes appear to combine to bring about an intentional shift in consciousness that is sufficiently atypical from ordinary consciousness and long-lasting enough to be considered an altered state.
Once activated, ordinary feelings of personal control are perceived by the healers as being replaced by a nonordinary sense of impersonal intentionality or passive volition; that is, from a gentle release of personal responsibility to a complete surrender of personal will.
As the healers proceed further into the "treatment" process they report that consciously directed thought processes become less the focus of attention. On the whole, these processes are surrendered during "treatment, " although not made entirely subordinate. Instead, rational conscious and nonrational subconscious processes appear to operate at first in an appositional relationship and then in an integrative, synergistic manner.
The healers claim that "expanded" awareness facilitates their increased access to subconscious materials. This may result in sudden intuitions (i.e., unconsciously processed "flashes" of information or awareness), symbols, and images that may seem to originate from beyond the self.
Due to the combined effects of sustained, absorbed attention and reduced sensory input from the external environment, body boundary awareness is reportedly decreased, and alterations in body image may be experienced.
In combination with the healer's ordinary identification with forces, energies, and/or spiritual or discarnate entities, alterations in body image are symptomatic of a weakening of the self-defining operations of the personal (or egoic) self in particular and the identity state (Tart, 1975a) in general.
Without the stabilizing effects of the self-system, the perceptual field may undergo modification, leading to an alteration in the generalized reality orientation (Shor, 1972) which, when coupled with alterations in the sense of self and cognitive processes, may be experienced as a general "existential shift" (Ehrenwald, 1978) into a mythic, or metaphorical, reality shaped by the healer's projected conscious and unconscious beliefs (see Larsen, 1988).
DISCUSSION The Dynamics of Transpersonal Healing The findings of this research suggest that the fundamental processes in transpersonal healing involve alterations in consciousness that are induced and amplified by the healer's conscious self-regulation of attention, physiology, and cognitive processes and shaped into a mythic reality based upon personal attitudes, goals, and system of beliefs. According to the healers, the induction of nonordinary consciousness results in an ascendance of ordinarily subconscious primary processes, producing modifications in ordinary temporal and spatial orientation, meanings, emotional responsiveness, and motor activity. These contribute additively toward a global alteration in one's sense of self as part of an ontological change marked by an increased uncritical acceptance of alternative reality configurations and a purported increase in the occurrence of parapsychological events. This may be interpreted as an alteration in the generalized reality orientation (Shor, 1972), "the structured frame of reference in the background of attention which supports, interprets, and gives meaning to all experiences" (p. 242). Although transpersonal healers generally emphasize intentionality as a conscious attempt to heal or set goals, subtle subconscious alterations of awareness appear to precede conscious intent. These psychophysiological changes constitute an experiential substrate that is potentiated more fully when meditative, self-regulative techniques and cognitive changes are applied; this appears to mobilize a departure from ordinary physiological operations and consciousness, establishing the intrapersonal conditions (e.g., sensations and perceptions) that healers associate with healing/influencing and may be identified by the healer as his or her "healing state." Conscious applications of self-regulative techniques seem to potentiate a preparatory set. Healers report that initially, and with some effort, they concentrate attention toward a single focus. Often, this is described as a physical sensation and/or process and/or a cognitive representation of the healee. Metaphorical (i.e., symbolic, mythic) constructs are used to augment the healer's ordinary concepts of reality (LeShan, 1990) and self, extending them beyond cultural, social, and personally-conditioned definitions and limits. This process bears some similarity to the synergic comparative mode of thinking described by Samples (1976):
Sustained concentration appears to result in an abatement of reflective self-awareness and the dissolution of self-other boundaries, and it leads toward greater involvement with, or absorption within, the object of attention. These processes are part of a transition from personal, egoically directed attention towards a less focused, more impersonal, detached, and "expanded" transpersonal awareness. The egoic self, that is, the self-as-construct, undergoes transformation as self-stabilizing, self-reflective cognitive processing abates. There is an awareness of appositional cognitive processes and the emergence of an ego-dystonic co-consciousness (see Prince in M�nsterberg, Ribot, Janet, Jastrow, Hart, & Prince [1910], pp. 71-101). The latter may be experienced as an undefined and impersonal "self" or "presence" upon which are projected characteristics arising from the healer's personal and/or cultural beliefs. The induction of altered, mythic, or shamanic (Hamer, 1982) consciousness effects a transformation in the individual's ontological and metaphysical orientations. This is referenced by alterations in the sense of identity (or "existential self" [Peters, 1989]) and one's changed relationship towards the altered physical reality. Healers describe how attention is directed away from cognitive systems supporting the ordinary self-construct (or identity state), including the physical and the personal (or "biographical" [Grof, 1985]) self that is maintained through memory and serves as an index against which one compares his or her present state of being. Thus, the existential changes produced through the healer's absorption within a metaphorical, or mythic, reality is the sine qua non of transpersonal healing: This is supported by the healers' ranked averages of significant experiential areas. Taxonomy A taxonomy of transpersonal healers was developed on the basis of the research findings. Figure I presents a distribution of the 20 transpersonal healers whose experiences were analyzed in this research. The legend displays the variety of healing types with which these individuals identify (refer to Tables I & 2). This includes 4 spiritual healers and 2 psychic healers who, based upon their sharing of a common designation, should fall into the same category.
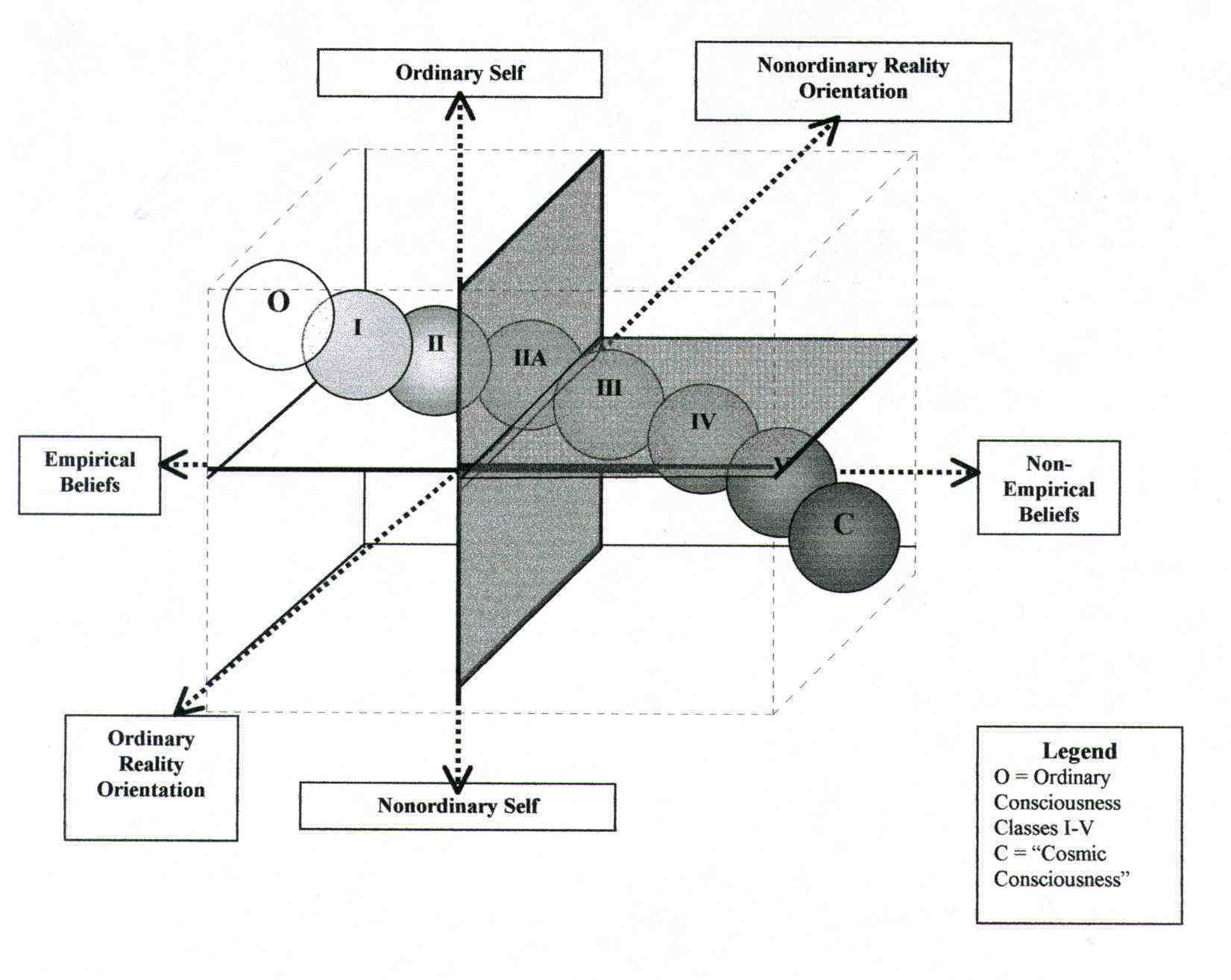
Fig. 1. Distribution and taxonomic classification of 20 transpersonal healers based upon estimates of level of consciousness and the structure of metaphorical constructs derived from content analysis and interview materials Based upon an analysis of ITHE scores and responses, the healers' configurations of consciousness (i.e., external reality-testing, sense of self, and metaphysical shift) were plotted against the types of metaphorical constructs used. Although healers generally implement a range of beliefs (as indicated by the horizontal bars intersecting with the circles), only those that are central to their efforts (represented by the circles) are used in the plotting. It is assumed that the stabilizing and organizing functions of the self-system in relation to physical and social realities plays a major role in maintaining and governing the configuration of ordinary consciousness (Tart, 1975a). Intermediate consciousness represents a less extreme stage lying between ordinary and altered consciousness, in which various features of ordinary and nonordinary consciousness co-exist in varying proportions. The predominant features distinguishing the three levels of consciousness is the degree of alteration in the sense of self, including personal identity. Within ordinary consciousness, self-awareness is generally intact. At the level of intermediate consciousness, the external reality-testing of the perceiving (egoic) self is weakened, but is present at points during the process. As a result, experients reported awareness of features of ordinary consciousness juxtaposed against aspects of nonordinary consciousness. At the level of altered consciousness, a complete breakdown of the self-other boundary is usually experienced, with a concomitant loss of self (awareness) associated with total absorption into an alternate metaphysical reality and/or metaphorical construct. The metaphorical constructs used by transpersonal healers are categorized into those that are realistic, metaphysical, and quasi-realistic. Realistic constructs conform closely with objects/energies in physical reality (e.g., referring to healing "energy" as akin to magnetism, electricity, or other known energies, or designating a specific object [e.g., the spine] as a source of "energy"). The polar opposite involves metaphysical (mythic, spiritual, and religious) constructs and symbols (e.g., "divine intelligence," "God's healing power," entering into a communion [or "merging"] with a deity in order to serve as a channel for information and "energy"). The quasi-realistic category includes a variety of hybrid constructs used to synthesize the disparity between the two poles (e.g., "psychic energy," discarnate guidance of "energy" or interventions, transfer of "energy," chakras, spirit guides). All categories refer to metaphors in the sense that they represent meaningful belief constructs expressed as figures of speech "in which one thing is likened to another, different thing by being spoken of as if it were that other" (Webster's Deluxe Unabridged, 1983, p. 1132). The types of metaphor differ, however, in terms of their being proximal or distal to conventional culturally shared and validated beliefs. Reality-based metaphors, for example, are referents designating one or more aspects of physical reality. These denote some type of healing-related "energy," force, or object that is based, with a greater or lesser degree of conformity, upon objects or concepts found within the consensual world view. Although they allude to "real" objects and/or energies, these metaphors are focused, discrete, and function representationally as signs, which convey nonabstracted information and meaning (Mowrer, 1963). In contrast, metaphysical metaphors, by virtue of their abstraction, appear to operate as symbols. They tend to be more conceptually remote from ordinary physical reality and refer to profound, expansive, and complex meanings extending beyond the forms in which they are expressed to the conscious mind. Quasi-realistic metaphors tend to reconcile the disparity existing between physical and metaphysical concepts. They are often characterized by (a) constructs offering explanations that betoken a reduced dependency upon physical reality, emphasizing special abilities or traits (e.g., "psychic" healing, "merging" with the healee, the transmission of nonphysical "energy"), and/or those (b) that involve a syncretic fusion (Werner, 1980) of features related to the realistic and metaphysical categories (e.g., discarnate guides are believed to be "real" individuals who once existed in physical reality but now exist in a spiritual realm or an alternate reality). A curvilinear relationship between the healers' level of consciousness and types of metaphorical constructs used is indicated. The arc connecting classes 1 through 5 suggests that the configurations of consciousness associated with transpersonal healing exist as discrete states distributed along a continuum from those that are most dependent upon ordinary (or nonordinary) consciousness and rely upon realistic and quasi-realistic constructs to those in which consciousness is extensively altered, and metaphysical (spiritual, religious) beliefs are emphasized. Using these two types of metaphorical constructs as coordinates, six healing types are identified. Classes of Healers Class I (n = 4). This cluster includes individuals who identify themselves as a magnetic healer, psychic healer, a transmitter of universal energy, and a practitioner of laying on of hands. They (a) rely upon rational processes to "treat" and explain their behaviors, (b) maintain ordinary (or near-ordinary) consciousness, and (c) maintain an ordinary sense of self during treatment. Although they stress reality-based constructs, quasi-realistic constructs are depended upon most heavily. They are not adverse to supporting the notion that subconscious operations play some role in the healing process (e.g., MacManaway with Turcan, 1983, pp. 64-67), although still emphasizing the role of conscious, rational processes. Class I healers are expected to rely most heavily upon physical (focusing) devices to supplement or amplify their healing treatment and diagnosis (e.g., use of the hands to direct energy, dowsing devices, crystals, etc.). Class 2 (n = 6). This group consists of a transformational healer, psychic healer, spiritual healer, energy healer, and therapeutic touch healer. As in Class 1, although Class 2 individuals combine realistic, quasi-realistic, and metaphysical beliefs (and/or images), they are less likely to rely upon physical objects (e.g., pendulums or crystals). However, Class 2 healers may use their hands to focus and "sense." They also differ from Class I in their more extensive moderate-to-extreme alterations of consciousness (including the sense of self). An effort is made to access unconscious processes for diagnosis and treatment. This group often reports transegoic threshold, or "access level," phenomena (e.g., feelings of a presence or co-consciousness). Egoic operations are present, although weakened, and may be reported as apposing subconscious processes. Class 2a (n = 2). These individuals include a LeShan Type I healer and a natural healer. As in Class 2, they report moderate-to-extreme alterations in consciousness, but emphasize nonreality-based (abstract, formless) and nonspiritual constructs (e.g., "merging" and "allowing") without relying upon quasi-sensory imagery. Whereas Class 2 healers incorporate mediational constructs (e.g., chakras and energy meridians) that frame and shape their experience, 2a individuals seem to be a special case of Class 2, describing what appears, at first, to be a "mythless" healing experience. Class 2a is characterized by healers' attempts to suspend beliefs in both physical and metaphysical metaphors and to not utilize mythic beliefs. However, belief in consciousness (as an extended, nonlocal entity) and "merging" (as an ability presumed to facilitate healing) remain fundamental to their practices. Class 2a is, therefore, less dependent on physical and spiritual constructs than Class 2, but more grounded in personal experience and a belief in special abilities. Class 3 (n = 2). Class 3 includes a spirit healer and a spiritual healer. Both undergo extensive transegoic alterations of consciousness and emphasize both realistic and quasi-realistic constructs, although expressed beliefs may run the gamut from reality based to spiritual (nonreality based). Spiritistic beliefs and mediumistic behaviors are highlighted here and may be used in healing efforts by channeling energy and/or receiving spirit guidance for diagnosis and treatment. One individual (Worrall) experienced mediumistic phenomena prior to her "intuitive" healing experiences; the other (Edwards, 1945) received training in mediumistic practices, but later (Edwards, 1971) disavowed the need for a trance state in healing. Class 4 (n = 2). Unlike Class 1, healers in Class 4 claim to transfer energy through full identification with a quasi-realistic energy. Although this is the primary method, they may identify with the healee at times during treatment. Their experience is characterized by an extensive transegoic alteration of consciousness and a complete loss of self. Class 5 (n = 4). This group includes a Christian Science healer, a Science of Mind healer, and two "spiritual healers." Transegoic consciousness is induced, and quasi-realistic (e.g., energy) and metaphysical (i.e., unstructured, nonreality-based) constructs are blended. Although spiritual healers combine quasi-realistic constructs with nonreality-based constructs, the combination produces the most unstructured and conceptually remote cognition to be found among all groups. A Continuum of Consciousness Figure 2 presents the five classes (and one subclass) of healers placed within a three-dimensional context based upon (a) the type(s) of metaphorical (or mythic) constructs used, (b) the generalized reality orientation (Shor, 1972), and (c) the healers' experienced sense of self. Figure 2. Conceptualized Plot in 3-dimensional Space of 6 Healer Types in Contrast to Ordinary and "Cosmic" Consciousness. Ordinary and cosmic consciousness (Bucke, 1961) are used as points against which changes in the healers' consciousness are referenced. Cosmic consciousness is described as an expanded, nirvana-like awareness that transcends self-consciousness. It has as its prime characteristics
Class I healers experience minimal changes in consciousness, emphasize more reality-based constructs than do the other classes, and maintain an ordinary (or near-ordinary) sense of self. Proceeding along the continuum, Classes 2 and 2a are intermediate in their use of metaphorical constructs and increased alteration in the generalized reality-orientation and sense of self. Classes 3, 4, and 5 undergo the most radical changes towards non-egoic operations and absorption within an alternate (mythical, metaphysical) reality. The Shamanic Complex and Inherency Shamanism is the concept that is most closely represented by the findings of this research (see Halifax, 1982; Larsen, 1988). The shamanic capacity to transcend the personal self, to enter into multiform identifications, to access and synthesize alternate perspectives and realities, and to find solutions and acquire extraordinary abilities used to aid the community bears a remarkable resemblance to transpersonal healing experiences. Webster's New World Dictionary (1970) defines a complex as "a group of interrelated ideas, activities . . . viewed as forming a single whole" [italics added] (p. 290). When Halifax (1979) refers to shamanism as an ecstatic religious complex, she uses this sense of the word "complex" to designate systems of behaviors and psychological characteristics that have survived over millennia and are found, in remarkably similar forms, throughout the world. Winkelman (1984) uses the term "shamanic complex" in association with the status, beliefs, roles, and activities of shamanic practitioners that are organized about a single role or category (p. 250). In this research, however, the meanings of "complex" stated above are synthesized with the Jungian (Jung, 1970) sense of the term, supplementing Halifax's (1979) and Winkelman's (1984) definitions by adding the notion of inherency: A complex is a multileveled construct that refers to behaviors, feelings, roles, thoughts, and perceptions constellated about, and expressive of, a central, inherent tendency (or instinct), the emergence of which is shaped by an interaction of personal and sociocultural structures, needs, conditions, and demands. Instincts are universal, sequential, species-specific patterns of adaption (Munn, 1965). In humans, they are purportedly experienced as somatic manifestations providing the drive that directs an individual's aim towards an object or consummatory act that facilitates tension-reduction (Freud, 1924/1956). Tension-reducing behaviors are expressed in the form of nonacquired, or unlearned, adaptive behaviors (Lorenz, 1981). The unpremeditated, reflexive mystical experiences of Deikman's (1972a) untrained-sensates involve the discharge of an organismic response through an encounter with nature or a drug experience. These events are characterized by involuntary alterations of consciousness, altered perception of one's relationship to the world and one's body, fleeting changes in one's sense of identity, and "expanded" awareness. Although these features are similar to those reported by trained mystics, they do not result from disciplined meditation or prayer and do not conform to any specific philosophical cosmology. No action is taken, nor is an action mode a common feature of the experience: It is primarily an altered, receptive mode of processing (Deikman, 1973), not easily explainable through conditioning or expectations, but possibly an inadvertent activation of the first phase of an endogenous potential in a situation lacking demand characteristics (also see Irwin, 1985b, for references to spontaneous extrasensory experiences and percipients' possible need for absorbed mentation [p. 7]). Incidents of instinctive, or intuitive, healing (Krippner, 1980) also occur spontaneously among naive, untrained children (Worrall & Worrall, 1965) and adults (G. Ille, personal communication, January 7, 1988; Kraft, 198 1; MacManaway with Turcan, 1983). The features of the onset (receptive) phase are similar to those found with Deikman's (1972a) untrained sensates, differing, however, in their (a) activation by an intense object relationship that effects a strong (b) emotional-loving and/or sympathetic-response that is accompanied by (c) somatic sensations of tingling or heat in one's hands and the (d) need or drive to extend one's ordinary limits and abilities in order to alleviate the suffering of the object of attention. The drive to relieve is frustrated by a sense of helplessness that is transcended through the healer's surrender of personal control and setting aside of reality limits, allowing the expression of unlearned, nonacquired, cognitive and/or motor behaviors, an organismic response that is usually combined with wish-fulfilling thinking. This is illustrated by an interviewee's statement:
The various overt or covert active efforts in healing-from intense wishing or prayer to touching, stroking, or laying on of hands (and/or other substances-unfold instinctively, unpremeditatively, and (consciously) unstructured by prior teachings or latent learning. There as a sense of direction from an internal source of guidance that is experienced as foreign to one's ordinary self. Drive reduction and reduced somatic sensations signal that the need has been satisfied. At times there is an intuitive sense of whether the effort was successful. The desired traits of shaman initiates vary from culture to culture. Recruitment is often based upon heredity (Eliade, 1951/1974), but selection may also be made through the cultural interpretation of signs from gods, epileptoid tendencies (see Winkelman, 1984), or hysterical traits. Shamanic behaviors have been associated with neurosis (Devereux, 1961), psychosis (e.g., schizophrenia, see Silverman, 1967), and hysteroid tendencies (see Radin, 1937) such as (a) emotional lability, (b) extreme sensitivity of contact with object reality, (c) ease of regression and "nervousness," (d) excitability, (e) ease of dissociation (i.e., trance states, depersonalization, amnesia), (f) role-playing behaviors (Page, 197 1), (g) somatization (i.e., the somatic expression of symbolic, unconscious, intrapsychic processes/conflicts [Cameron, 1963]), and (h) loose intrapsychic organization due to the lack of a consistent, integrative identity. Thus, in some societies the shamanic candidate may be identified by the characteristics associated with an inherently unstable sense of identity and ease of regression followed by the accession of subconscious processes, contents, and abilities:
The presence or level of pathology, however, cannot be inferred simply on the basis of field reports alone. In a study of Apache shamans, Boyer, Klopfer, Brawer, and Kawai (1964) analyzed Rorschach protocols gathered from 12 Apache shamans, 52 nonshamans, and 7 pseudoshamans (i.e., individuals whose claims of shamanic powers did not result in their being accorded the status of shaman in their culture). They found that the shamans' reality testing and approach toward ambiguous stimuli was equivalent to that of the nonshamanic group. Shamans, however, provided indications suggesting a greater ease of regression, greater awareness, more tolerance of ambiguity, and a stronger orientation towards theoretical thinking. Although the shamans' test protocols provided indications suggestive of clinical hysteria, the authors conclude that behaviorally, shamans appeared less hysterical and demonstrated a state of mental and emotional health that was greater than members of the other groups (also see Boyer, Boyer, & DeVos, 1982). Following selection, shaman initiates undergo an educational indoctrination in the metaphysics of the culture (including its transpersonal symbols [see Assagioli, 19691). They learn the techniques of ecstasy (i.e., the induction of altered consciousness); the identities and powers of helping and harmful spirits; magical, divinatory, and healing methods; and the society's mythic cosmology. During the experiential phase, however, the trainee is guided towards fully experiencing an initiatory "death" of self, a powerful, ontologically transforming experience:
Access to transpersonal consciousness is inaugurated by the shaman initiate's ego-death, potentiating the ability for magical flight into mythic realms on an inner journey (through absorbed involvement) into projections of cultural belief (see Larsen, 1988). Upon completion, or "rebirth," the consciousness of the initiate is reintegrated and transformed in a manner similar to that described above. Hence through controlled regression and the ascendance and integration of subconscious materials, the initiate moves closer to the ability to intentionally access magical/healing/divining powers not available in ordinary (e.g., nonshamanic) consciousness. In outline, the essence of the shamanic complex includes features that are strikingly similar to those found in transpersonal healing: 1.The shaman mobilizes a preparatory set by establishing functionally determined conditions under which his or her intent is expected to manifest. Generally, these contexts take the form of rituals and ceremonies during which symbols associated with the shaman's helping spirit aid in his or her identification with the spirit's powers to escape the confines of the profane world and enter into "sacred time" and its associated mythic reality. 2.Consciousness is intentionally altered through a variety of means, including rhythmic dancing, drumming, chanting, and/or the use of hallucinogenic drugs. 3.Through the alteration of consciousness, the shaman's ordinary sense of self is changed, and he or she enters into an intense, mystical identification with guardian spirits that guide his or her travels through the projected, alternate realities constructed from the culture's mythology; the combination of factors effectively modifies the shaman's metaphysical orientation and operations. By assuming an alternate identity (or "alter ego"), the shaman acquires nonordinary abilities within the rituals, some of which remain after completion of the "journey. " Thus, the shamanic complex is more than an "ecstatic religious complex of particular and fixed elements with a specific ideology" (Halifax, 1979, p. 3). It appears to have a transpersonal, transcultural, psychological, and physiological infrastructure underlying the different methods, beliefs, and contexts within which such an inherent tendency is activated: "The inherent psychobiological predisposition to achieve the [Shamanic State of Consciousness] is not culture bound and is perhaps universal in the species" (Noll, 1983, p. 444). The Shamanic Roots of Transpersonal Healing Like shamans, trained transpersonal healers establish a preparatory set, voluntarily alter their consciousness, diminish their ordinary sense of self, and identify with mythic constructs. Transpersonal healers differ, however, in their personal selection of mediational constructs from among the heterogeneous beliefs found in Western societies, rather than adopting those that are consonant with an overarching cultural paradigm. The selected constructs appear to offer the most meaningful interpretation and integration of the healing/influencing phenomena. The transpersonal healers studied here also differ in the complete absence of shamanic "flights." This may be explained as a function of their commitment to (or indoctrination in) the mythos of a culture and/or subculture that neither supports the concept of "flight" nor offers a cosmological "map" necessary for such travels. Shamanic-like "flights" may be represented, however, in nonhealing-related ecsomatic experiences, such as near-death experiences (Moody, 1975), traveling clairvoyance (Grof, 1988), and out-of-body experiences (Irwin, 1985a; Monroe, 1971). Thus, transpersonal healing appears to be a contemporary adaptation of the shamanic complex, a core process from which the variety of transpersonal healing methods evolved. Hypothetically, the endogenous or "instinctive" tendency (proposed earlier) about which these behaviors and ideologies are constellated may be a psychophysiological potential that, when activated, effects a shift towards decreased sympathetic arousal, increased parasympathetic activity, and a shift away from ordinary cerebral activities: (a) reduced control of the dominant, verbal-analytic hemisphere and asynchronous EEG activity (Ehrenwald, 1978) and (b) increased hemispheric equivalence as indicated by (c) greater hemispheric synchronization (Cade, 1976; Cade & Coxhead, 1979; Don, McDonough, & Warren, 1989; Millay, 1981), and (d) the production of specific power spectra that may be related to purported healing/influencing or psi phenomena (Cade & Coxhead, 1979; Don, McDonough, Collura, & Warren, 1988; Whitton, 1974). The reduced activity of the dominant hemisphere may be a precursor to the appearance of hemispheric synchronization and changes in power spectra. Similarly, Winkelman (1984) hypothesizes that the methods used to alter consciousness among magico-religious practitioners may produce a trophotrophic response, hemispheric synchronization, and parasympathetic nervous system dominance "in which the frontal cortex is dominated by slow wave patterns originating in the lower centers of the brain" (pp. 145-146). Although most of Winkelman's features presumably might be found in the majority of transpersonal healers participating in this research, the last characteristic-slow wave patterns-is contradicted by the EEG analysis of Krieger's cerebral activity during therapeutic touch (Krieger, Peper, & Ancoli, 1979). It should be recalled, however, that two healers provide descriptions suggesting that arousal level (or sympathetic dominance) is increased; this hyperarousal may, however, lead to a physiological collapse and the onset of a trophotrophic state (Fischer, 1986). Hence Krieger's EEG data, in combination with the two healers who reported increased arousal, may provide indications of at least two variants in a possible range of physiological patterns among transpersonal healers that merits further investigation.
CONCLUSIONS For almost three decades, a considerable body of literature involving experimental investigations of transpersonal healing effects has accumulated. The data suggest the existence of an anomalous healing/influencing process that may be potentiated by transpersonal healers, as well as naive individuals, under controlled conditions (e.g., Nash, 1982, 1984). Although provocative, the results presented here are provisional and require further empirical investigation and refinement. The data are based upon systematically gathered and analyzed reports of personal experience among transpersonal healers; they require correlation with verified healing effects. The data suggest, however, that the traditional methods of classifying transpersonal healing types may be refined by developing a process based (rather than context-based) systems approach. Transpersonal healers (as well as indigenous healers, parapsychological subjects, etc.) may be classified according to modifications in their systems of consciousness in combination with other psychological, psychophysiological, and sociocultural variables. The motivational source of anomalous healing may lie within an endogenous, organismic thrust towards holistic functioning. This must be examined more intensively if the operations of healing/influencing are to be understood. The scientific preoccupation with the control and measurement of empirical effects must be counterbalanced by providing equal attention to investigations of the psychological and physiological processes of healers and healees (or target materials). The interpersonal, or social/ environmental, climate within which positive and negative effects occur requires more intensive scrutiny, and the physical medium(s), if any, through which these effects are mediated should be explored. Holistic research of this type requires that the healing/influencing setting, whether field or laboratory, should be treated as a complete system, a comprehensive process requiring the equal distribution of researchers' attention towards physical, psychological, and parapsychological aspects (Krippner & Villoldo, 1976) and not the control and measurement of physical effects alone.
ASSAGIOLI, R. (1969). Symbols of transpersonal experiences. Journal of Transpersonal Psychology, 1, 33-45. BEARD, R. (1951). Everyman's Search. Worcestershire, England: Arthur James. BOYER, L. B., KLOPFER, B., BRAWER, F. B., & KAWAI, H. (1964). Comparisons of the shamans and pseudoshamans of the Apaches of the Mescalero Indian reservation: A Rorschach study. Journal of Projective Techniques, 28, 173-180. BOYER, L. B., BOYER, R. M., & DEVOS, G. A. (1982). An Apache woman's account of her recent acquisition of the shamanistic status. Journal of Psychoanalytic Anthropology, 5, 299- 331. BRAUD, W. G. (1978). Allobiofeedback: Immediate feedback for a psychokinetic influence upon another person's physiology [Summary]. In W. G. Roll (Ed.), Research in Parapsychology 1977 (pp. 123-134). Metuchen, NJ: Scarecrow. BRAUD, W., & SCHLITZ, M. (1983). Psychokinetic influence on electrodermal activity. Journal of Parapsychology, 47, 95-119. BRAUD, W., & SCHLITZ, M. (1989). A methodology for the objective study of transpersonal imagery. Journal of Scientific Exploration, 1, 43-63. BUCKE, R. M. (1961). Cosmic Consciousness: A Study in the Evolution of the Human Mind. Secaucus, NJ: Citadel. Cade, C. M. (1976). Biofeedback as an aid to self-control of internal states. Surrey, England: The Radionic Association. CADE, C. M., & COXHEAD, N. (1979). The Awakened Mind. New York:Delacorte. CAMERON, N. (1963). Personality Development and Psychopathology. Boston: Houghton Mifflin. CHAPMAN, G., WITH STEMMAN, R. (1984). Surgeon From Another World (rev. ed.). Wellingborough, Northamptonshire, England: Aquarian. CHEIN, I. (1981). Appendix: An introduction to sampling. In L. H. Kidder, Research Methods in Social Relations (4th ed.) (pp. 418-441). New York: Holt, Rinehart, & Winston. COLLEN, A. (1984). Overview of Methods for Disciplined Inquiry. San Francisco: Saybrook Institute. COOPERSTEIN, M. A. (1985). Creativity and consciousness. Saybrook Review, 5(2), 28-36. COOPERSTEIN, M. A. (1990). The Myths of Healing: A Descriptive Analysis and Taxonomy of Transpersonal Healing Experience. Unpublished doctoral dissertation, Saybrook Institute, San Francisco, CA. DEAN, E. D. (1983). An Examination of Infra-Red and Ultra-Violet Techniques to Test for changes in Water Following the Laying-on-of-Hands. Unpublished doctoral dissertation, Saybrook Institute, San Francisco, CA. DEAN, E. D., & BRAME, E. (1975). Physical changes in water by laying on of hands. Proceedings of the Second International Congress on Psychotronic Research (pp. 200-202). DEIKMAN, A. J. (1972a). Deautomatization and the mystic experience. In C. T. Tart (Ed.), Altered States of Consciousness (pp. 25-46). Garden City, NY: Anchor. DEIKMAN, A. J. (1972b). Experimental meditation. In C. T. Tart (Ed.), Altered States of Consciousness (pp. 203-223). Garden City, NY: Anchor. DEIKMAN, A. J. (1973). Bimodal consciousness. In R. E. Ornstein (Ed.), The Nature of Human Consciousness (pp. 67-86). New York: Viking. DEVEREUX, G. (1961). Shamans as neurotics. American Anthropologist, 63, 1088-1090. DON, N. S., WARREN, C. A., McDONOUGH, B. E., & COLLURA, T. F. (1988). Event-related brain potentials and a phenomenological model of psi-conducive states [Summary]. In D. H. Weiner & R. L. Morris (Eds.), Research in Parapsychology 1987 (pp. 72-76). Metuchen, NJ: Scarecrow. DON, N. S., McDONOUGH, B. E., & WARREN, C. A. (1990). EEG effects associated with psi-hitting and psi-missing in a token-object task [Summary]. In L. A. Henkel & J. Palmer (Eds.), Research in Parapsychology 1989 (pp. 53-57). Metuchen, NJ: Scarecrow. EDDY, M. B. (1971). Science and Health with Key to the Scriptures. Boston: First Church of Christ Scientist. (Original work published 1875) EDWARDS, H. (1945). The Science of Spirit Healing. London: Rider. EDWARDS, H. (I 971). The Healing Intelligence. New York: Taplinger. EHRENWALD, J. (1978). Psi phenomena, hemispheric dominance and the existential shift. In B. Shapin & L. Coly (Eds.), Psi and States Of Awareness (pp. 211-220). New York: Parapsychology Foundation. ELIADE, M. (1974). Shamanism: Archaic Techniques of Ecstasy (W. R.Trask, Trans.). Princeton, NJ: Princeton University Press. (Original work published 1951) FISCHER, R. (1986). Toward a neuroscience of self-experience and states of self-awareness and interpreting interpretations. In B. B. Wolman & M. Ullman (Eds.), Handbook of States of Consciousness (pp. 3-30). New York: Van Nostrand Reinhold. FREUD, S. (1956). A General Introduction to Psychoanalysis (J. Riviere, Trans.). Garden City, NY: Permabooks. (Original work published 1924) GEERTZ, C. (1973). The Interpretation of Cultures. New York: Basic Books. GRAD, B., CADORET, R. J., & PAUL, G. 1. (1961). An unorthodox method of treatment on wound healing in mice. International Journal of Parapsychology, 3(2), 5-24. GROF, S. (1985). Beyond the Brain. Albany: State University of New York Press. GROF, S. (1988). The Adventure of Self-Discovery. Albany: State University of New York Press. HALIFAX, J. (1979). Shamanic Voices: A Survey of Visionary Voices. New York: Dutton. HALIFAX, J. (1982). Shaman: The Wounded Healer. London: Thames & Hudson. HARNER, M. (1982). The Way of the Shaman: A Guide to Power and Healing. New York: Bantam. HOLMES, E. (1953). The Science of Mind. New York: Dodd, Mead. HUNT, V. V., MASSEY, W. W., WEINBERG, R., BRUYERE, R., & HAHN, P. M. (1977). A Study of Structural Integration From Neuromuscular, Energy Field, and Emotional Approaches [Summary]. Boulder, CO: Rolf Institute. IRWIN, H. J. (1985a). Flight of Mind: A Psychological Study of the Outof-Body Experience. Metuchen, NJ: Scarecrow. IRWIN, H. J. (1985b). Parapsychological phenomena and the absorption domain. Journal of the American Society for Psychical Research, 79, 1-11. Joy, W. B. (I 978). Joy's Way: A Map for the Transformational Journey. Los Angeles, CA: Tarcher. JUNG, C. G. (1970). Analytical Psychology. New York: Vintage. KMETZ, J. M. (1981). Appendix: Cell culture experiments with Dean Kraft. In D. Kraft, Portrait of a Psychic Healer (pp. 181-187). New York: Putnam's. KRAFT, D. (1981). Portrait of a Psychic Healer. New York: Putnam's. KRIEGER, D. (1979). The Therapeutic Touch: How to Use Your Hands to Help or to Heal. Englewood Cliffs, NJ: Prentice-Hall. KRIEGER, D., PEPER, E., & ANCOLI, S. (1979). Therapeutic touch: Searching for evidence of physiological change. American Journal of Nursing, 4, 66-62. KRIPPNER, S. (1980). A suggested typology of folk healing and its relevance for parapsychological investigation. Journal of the Society for Psychical Research, 50, 491-500. KRIPPNER, S., & VILLOLDO, A. (1976). The Realms of Healing. Millbrae, CA: Celestial Arts. LARSEN, S. (I 988). The Shaman's Doorway. Barrytown, NY: Station Hill. (Original work published 1976) LESHAN, L. (1969). Toward a General Theory of the Paranormal (Parapsychological Monographs No. 9). New York: Parapsychology Foundation. LESHAN, L. (1974). The Medium, the Mystic, and the Physicist. New York: Viking. LESHAN, L. (1990). Explanations of psychic healing. ASPR Newsletter, 16(l), 1-3. LIONBERGER, H. J. (1985). An Interpretive Study of Nurses' Practice of Therapeutic Touch. Unpublished doctoral dissertation, University of California, San Francisco. LORENZ, K. Z. (1981). The Foundations of Ethology (R. W. Kickert, Trans.). New York: Springer-Verlag. MACMANAWAY, B., WITH TURCAN, J. (1983). Healing: The Energy That Can Restore Health. Wellingborough, Northamptonshire, England: Thorsons. MCCALL, R. B. (1986). Fundamental Statistics for Psychology (4th ed.). New York: Harcourt Brace Jovanovich. MILLAY, J. (I 981). Brainwave synchronization: A study of subtle forms of communication. Humanistic Psychology Institute Review, 3(l), 9-40. MILLER, R. N. (1982). Study of remote mental healing. Medical Hypotheses, 8, 481-490. MONROE, R. A. (1971). Journeys Out of the Body. Garden City, NY: Doubleday. MOODY, R. A., JR. (1975). Life After Life? Atlanta, GA: Mockingbird Books. MOWRER, 0. H. (1963). Learning Theory and the Symbolic Process. New York: Wiley. MUNN, N. L. (1965). The Evolution and Growth of Human Behavior (2nd ed.). Boston: Houghton Mifflin. M�NSTERBERG, H., RIBOT, T., JANET, P., JASTROW, J., HART, B., & PRINCE, M. (1910). Subconscious Phenomena. Boston: Gorham. NASH, C. B. (1982). Psychokinetic control of bacterial growth. Journal of the Society for Psychical Research, 51, 217-221. NASH, C. B. (1984). Test of psychokinetic control of bacterial mutation. Journal of the American Society for Psychical Research, 78, 145-152. NEHER, A. (1980). The Psychology of Transcendence. Englewood Cliffs, NJ:Prentice-Hall. NOLL, R. (1983). Shamanism and schizophrenia: A state-specific approach to the "schizophrenia metaphor" of shamanic states. American Ethnologist, 10, 443-459. Osis, K., BOKERT, E., & CARLSON, M. L. (1973). Dimensions of the meditative experience. Journal of Transpersonal Psychology, 5, 109-135. PAGE, J. D. (1971). Psychopathology. New York: Aldine-Atherton. PEKALA, R. J. (1985). A psychophenomenological approach to mapping and diagramming states of consciousness. Journal of Religion and Psychical Research, 8, 199-214. PEKALA, R. J., & LEVINE, R. L. (1981-82). Mapping consciousness: Development of an empirical-phenomenological approach. Imagination, Cognition and Personality, 1, 29-47. PEKALA, R. J., & WENGER, C. F. (1983). Retrospective phenomenological assessment: Mapping consciousness in reference to specific stimulus conditions. Journal of Mind and Behavior, 4, 247-274. PETERS, L. G. (1989). Shamanism: Phenomenology of a spiritual discipline. Journal of Transpersonal Psychology, 21, 115-137. POLKINGHORNE, D. (1983). Methodology for the Human Sciences: Systems of Inquiry. Albany: State University of New York Press. PUHARICH, H. K. (1974). Psychic research and the healing process. In E. D. Mitchell et al. (J. White, Ed.), Psychic Exploration: A Challenge for Science (pp. 333-347). New York: Putnam's. QUINN, J. F. (1982). An Investigation of the Effects of Therapeutic Touch Done Without Physical Contact on State Anxiety of Hospitalized Cardiovascular Patients. Unpublished doctoral dissertation, New York University, New York City, NY. RADIN, P. (1937). Primitive Religion: Its Nature and Origin. New York: Viking. RAUSCHER, E. A., & RUBIK, B. A. (1980). Effects on motility behavior and growth of Salmonella typhimurium in the presence of a psychic subject [Summary]. In W. G. Roll (Ed.), Research in Parapsychology 1979 (pp. 140-142). Metuchen, NJ: Scarecrow Press. RAUSCHER, E. A., & RUBIK, B. A. (1983). Human volitional effects on a model bacterial system. Psi Research, 2(l), 38-48. ROBERTS, T. B. (1981). Consciousness, psychology and education. Phoenix, 5, 79-116. ROSE, L. (1968). Faith Healing. London: Gollancz. SAMPLES, R. (1976). The Metamorphic Mind. Reading, MA: Addison Wesley. SANFORD, A. (1972). The Healing Light. St. Paul, MN: Macalester Park. SCHIEGL, H. (1987). Healing Magnetism: The Transference of Vital Force Through Polarity Therapy. London: Century. SCHWARTZ, S. A., DEMATTEI, R. J., BRAME, E. G., JR., & SPOTTISWOODE, S. J. P. (1986). Infrared Spectra Alteration in Water Proximate to the Palms of Therapeutic Practitioners. Los Angeles: Mobius Society. SHERWOOD, K. (1985). The Art of Spiritual Healing. St. Paul, MN: Llewellyn. SHOR, R. E. (1972). Hypnosis and the concept of the generalized reality orientation. In C. T. Tart (Ed.), Altered States of Consciousness (pp. 239-256). Garden City, NY: Anchor. SILVERMAN, J. (1967). Shamans and acute schizophrenia. American Anthropologist, 69, 21-31. SOLFVIN, J. (1984). Mental healing. In S. Krippner (Ed.), Advances in Parapsychological Research 4 (pp. 31-63). Jefferson, NC: McFarland. STANFORD, R. G. (1977). Experimental psychokinesis: A review from diverse perspectives. In B. B. Wolman (Ed.), Handbook of Parapsychology (pp. 324-381). New York: Van Nostrand Reinhold. TART, C. T. (1975a). States of Consciousness. New York: Dutton. TART, C. T. (Ed.). (1975b). Transpersonal Psychologies. New York: Harper & Row. Webster's Deluxe Unabridged Dictionary. (1983) (J. L. McKechnie, Ed.). New York: Dorset & Baber. Webster's New World Dictionary of the American Language.(1970)(D. B. Guralnik, Ed.). New York: World. WERNER, H. (1980). Comparative Psychology of Mental Development (rev. ed.). New York: International Universities Press. (Original work published 1940) WHITTON, J. L. (1974). "Ramp functions" in EEG power spectra during actual or attempted paranormal events. New Horizons, 1,174-183. WINKELMAN, M. (1984). A Cross-Cultural Study of Magico-Religious Practitioners. Unpublished doctoral dissertation, University of California, Irvine. WORRALL, A. A., & WORRALL, 0. N. (1965). The Gift of Healing: A Personal Story of Spiritual Healing. New York: Harper & Row.
|
|
Medical Disclaimer: This website is underwritten completely by Dr. Cooperstein.
The purpose of the content is to educate, inform and
recommend. Under no circumstances is it meant to replace the expert care and
advice of a qualified professional as rapid advances in medicine may cause
information to become outdated, invalid or subject to debate. Accuracy
cannot be guaranteed.
Dr. Cooperstein
assumes no responsibility for how information,
products and books presented are used and
does not warrant
or guarantee the content, accuracy or veracity of any linked sites. Dr.
Cooperstein makes no guarantee to any representations made by listings
in professionals or support services directories.
|