|
|
|
|
|
|
See Example of a Disability Examination SAMPLE:
EXTRACTED INDEPENDENT PSYCHOLOGICAL EXAMINATION 2 M. Allan Cooperstein, Ph.D.
I. Purpose of examination: A. Mrs. Smith requested a psychological examination to review all case materials, assess her and render an objective, professional opinion regarding her emotional status. I explained the difference between the role of an Independent Medical Examiner and that of a treating psychologist. She elected to implement my services in the first capacity. B. She was told the purpose of the examination and indicated that she understood the examination was set within a legal context, that no patient/physician confidentiality or treatment was involved and assumed personal liability for my fees irrespective of the examination outcome and opinion.
TESTS/PROCEDURES (Omitted)
II.
Records Reviewed
B.
Ms. Montego -- audiology --
March 11, 1997 ENG:
C.
Dr. Garcia -- Neuro-ophthalmologist
-- March 19, 1997 D. Dr.Cochran -- cerebral MRI -- April 3, 1997: Normal study.
E.
Dr. Garcia -- April 24,
1997
F.
Dr. Temple -- Neurology --
May 13, 1997
G.
Ms. Martin -- Audiology --
May 13, 1997
H.
Dr. Hand -- Optometry --
July 17, 1997
I.
Dr. Hand -- July 15, 1997
J.
Dr. Garcia -- December 4,
1997
K.
Dr. Joseph Mildow --
December 10, 16 22, 1997
L.
Nancy Weiss -- Audiologist
(faxed comments dated March 31, 1997)
M.
Joseph M. Bartle, M.D.--
Pennsylvania Bureau of Disability Determination Report-- February 19, 1998
N.
John Millar, MD Telephone
consult 4/7/98
O.
M. Faust, MD Neurotology
Abington College Department of Otorhinolaryngology: Head and Neck Surgery
7/14/98
P.
Neil Pettit, Ph.D. Professor &
Director of the Abington College School of Medicine Division of Audiology and
Hospital of the Abington College Speech-Language Pathology
III. PSYCHOLOGICAL testING
A.
Experiential
Index
B.
Psychiatric
Screening Profile
C. Psychogenic Health Analysis
D. Murray Personality Assessment
Summary: Patient is characteristically non--disclosing about emotions and weaknesses. Prone towards understatement and may minimize her actual physical or emotional needs. Personality traits indicate predominant dependency, hysteria and compulsive tendencies. Axis I syndromes indicates clear, clinical levels of anxiety and depression, with a tendency to somatize resulting from her internalization of emotions. Faced with interpersonal tensions, she tries to maintain an air of buoyancy, denying all disturbing emotions and concealing inner discomforts with short-lived pleasantries and enthusiasms. To secure strong dependency needs, this woman is has become exceedingly responsive to the needs of others. She seeks harmony with others, even at the expense of her views and beliefs. Basically unsure of her strengths and lacking in self-confidence--despite superficial appearances to the contrary--she seeks to avoid situations that may involve personal conflict, preferring to smooth matters over as best she can. She is experiencing clinical signs of generalized anxiety of an uncharacteristic nature. Agitated and apprehensive, she may report physical discomforts such as headaches, gastrointestinal symptoms, fatigue, insomnia, jitteriness and diffuse fears. Events of the recent past are likely to have prompted a dysthymic syndrome in this otherwise controlled woman who declines self-disclosure. A depressive pattern of diminished security and self-deprecation has emerged, especially in regard to matters of personal worth, effectiveness and physical attractiveness. E. Ramstead Health Inventory Another valid profile, Mrs. Smith is described as introversive yet showing confidence. NOTEWORTHY RESPONSES included HEALTH PREOCCUPATIONS PSYCHIATRIC POSSIBILITY DEPRESSIVE FEELINGS, but no ILLNESS OVERREACTIONS or (tendencies to magnify illness consequences) . F. Minnesota Multiphasic Personality Inventory-2 Validity scales are all within normal limits. She is experiencing low morale and a depressed mood. She is preoccupied with feeling guilty and unworthy. She feels regretful and unhappy about life, and seems plagued by anxiety and worry about the future. She feels hopeless at times and feels that she is condemned. She has difficulty managing routine affairs, and the item content she endorsed suggests a poor memory, concentration problems, and an inability to make decisions. She appears to be immobilized and withdrawn and has no energy for life. She views her physical health as failing and reports numerous somatic concerns. She feels that life is no longer worthwhile and that she is losing control of her thought processes. According to her self-report, there is a strong possibility that she has seriously contemplated suicide. She is rather high-strung and believes that she feels things more, or more intensely, than others do. She feels quite lonely and misunderstood at times. She views herself as having so many problems that she is no longer able to function effectively in day-to-day situations. Her low mood and pessimistic outlook on life weigh heavily on her and seemingly keep her from acting to better her situation. Her negative self-attitudes and sense of frustration may be very detrimental to treatment and require attention early in therapy. G. post traumatic stress disorder. Based upon the results of the MMPI 2,without revealing the purpose of the questioning, Mrs. Smith was asked to describe whether or not she experienced any of the symptoms of PTSD. She was positive for the following 11 of 17 symptoms of post traumatic stress disorder.
H.
Neuropsychological Screening
Analysis Response Bias: Reliability & Validity
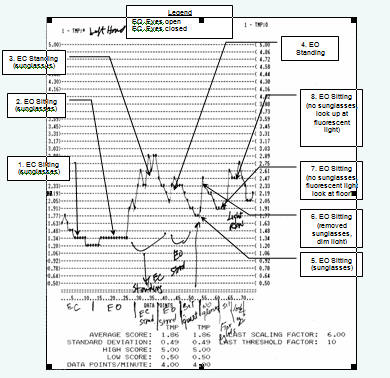
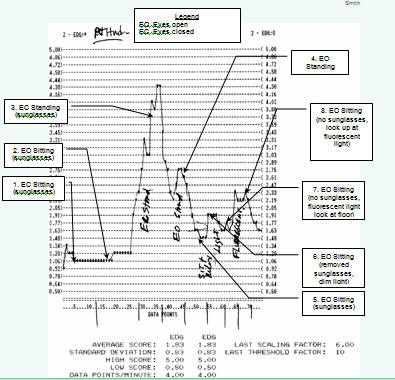
COMMENTS III. PSYCHOPHYSIOLOGY
A. PATIENT results
(Ranges/hemisphere)
B.
Procedure C. PHYSIOLOGICAL READINGS Part 1
1.
0-12 eyes closed
sitting Part 1 EDR RANGES
Average left 1. 86 mho
D.
Qualitative
Interpretation
4.
Permitting her to
sit and relax resulted in a noticeable decrease in reactivity.
IV.
MENTAL STATUS
2.
Mood and affect 3. Appropriateness: Appropriate. 4. Attitude/Manner: Cooperative, Direct, Rapport--Good, Resentful, Straightforward 5. Task Orientation: Attentive, Distractible, Scattered, Tired 6. Speech: Articulate, Detailed, Goal-Directed, Informative, Pressured, Self-Initiating, Talkative 7. Perceptual disturbances: None 8. Thought Processes: Thinking was largely logical, relevant and goal-oriented with indications of thought blocking and avoidance. 9. Content: Centered about the impact of her illness upon employment and its sequelae. 10. Alertness and level of consciousness: Alert. 11. Orientation: X 3 12. Memory: Long-term intact; short-term somewhat impaired due to emotional factors. 13. Concentration: Some impairment due to emotional reactions. 14. Abstract thinking: Appropriate for age and education. 15. Fund of information and intelligence: Appears of at least average intelligence with fund of information consistent with age and background. 16. Impulse control: Appears adequate. 17. Judgment and insight: Patient appears somewhat insightful; judgment is adequate. 18. Reliability: Patient assessed as reliable informant. V. DIAGNOSIS
VI. Summary A. Historically, Mrs. Smith has been an industrious worker and devoted mother. In addition, she was working towards an Associate's degree in insurance and holds an agent's license. B. Mrs. Smith has suffered from an unspecified viral infection that has afflicted her with photophobia, nystagmus, and vertigo. Consequently, she must avoid sunlight, wear dark glasses and rest extensively. She has continual pain in her eyes (and with eye movement), headaches, nausea, blurred vision, dizziness, pulsing in eyes, muscle tics, disequilibrium worsening later in the day. Occasional morning awakenings with dizziness. Highly sensitive to body movements and those of objects around her. C. Since my initial contact with Mrs. Smith, I have referred her for: 1. Neurophysiological testing 2. Audiological examination 3. Psychiatric/neuropsychiatric examination 4. Neurotological examination D. SUMMARY OF MEDICAL FINDINGS 1. OPTOMETRY a) Detached vitreous leading to conjunctivitis which became keratoconjunctivitis. b) Permanently scarred corneas. c) Alteration in eye dominance from right to left eye. This may have also caused a shift in her perceptual field contributing to her symptoms. d) Considered unemployable. 2. AUDIOLOGY a) Upbeating nystagmus with eyes closed. b) Brief upbeating nystagmus with changed direction of gaze from center to 30 degrees up. c) Severe, subjective vertigo immediately following the initial right Dix-Hallpike positioning. d) Positional testing was remarkable for upbeating nystagmus in the right lateral positions. e) Nystagmus may be associated with central dysfunction. f) Extreme nausea and dizziness following rotation and refused counter-clockwise stimulation. g) Normal peripheral hearing h) Bilateral reduced labyrinthine function. i) Spontaneous nystagmus induced after strain of 40 minutes of visual/auditory testing. 3. NEURO-OPTHALMOLOGY a) Viral keratoconjunctivitis in July, 1996, first in right eye, then left. b) Episodes of transient diplopia and impaired vision. c) Five changes in prescription. d) No longer able to read or carefully track with her eyes. Images become distorted, taking on different shapes. Reading up close, she becomes dizzy, feels off balance and slightly nauseated. Persistent pain in both eyes and sensitivity to light. When dizzy symptoms are at their worst, she feels as though she is leaning off to the left. e) Multiple subepithelial defects in right cornea. A few evident on the left. f) Normal mental status. g) The Romberg sign is said to be positive when unsteadiness is increased by closure of the eyes; the sign is present in diseases affecting the posterior column or polyneuritis in which there is loss of proprioception in the muscles of the lower extremities. The Romberg test is not performed when the patient has vestibular dysfunction or cerebellar disease with ataxia, because the results will obviously be positive. Romberg testing showed "quite a bit of swaying and fell to the left a few times." h) Visual distortions are likely related to cornea defects. i) Symptoms are referable to either a post- viral acute disseminated encephalomyelitis or a viral vestibulitus. ENG showed upbeat nystagmus with the eyes closed, a left deviation in right lateral position. 4. RADIOLOGY a) Normal MRI 5. NEUROLOGY a) Visual distortions explained due to corneal scarring. b) Vestibular rehabilitation recommended. 6. NEUROPHYSIOLOGY a) Pre-and post chiasmal potentials normal. Twenty channel topography normal. Digital EEG normal. BAEP, P300 normal. 7. PSYCHIATRY a) Dr. Bartle: (1) No prior psychiatric involvement. (2) Could not retain balance with eyes closed (this corresponds with my observations and the Romberg test). (3) Good informant. (4) Difficulty concentrating and grasping the meaning of what she is reading. (5) Axis I diagnosis of Adjustment Disorder, Depressed Affect and Axis III pathology of the eyes and neurological deficits of undetermined origin. (6) Patient severely stressed by circumstances, not know what is wrong with her, physicians have not been able to definitively diagnose condition. b) Dr. Millar (1) Major Depression with symptoms of PTSD (2) Subclinical personality features exacerbated by Axis III conditions. 8. NEUROTOLOGY a) Psychogenic dizziness associated with chronic anxiety, panic and phobia. b) No objective evidence of peripheral vestibular system or central vestibular system involvement at present. c) Abnormal control of maintenance of upright stance in the sagittal plane as found in individuals with significant psychologic overlays. d) It is reasonable to consider an initial viral insult secondary to other evidence of viral infection that was occurring at the time causing insult to the vestibular portion of the inner ear. While not ongoing, the damage may then cause symptoms when head movements are made. e) Significant reactions as depression, anxiety, and panic, can disrupt the normal compensation process and create a significant exacerbation to minor symptoms with ongoing head movements. f) Vestibular rehabilitation therapy is appropriate for helping to habituate the responses to head movements. However, in this case it would be adjunctive to behavioral, psychological, and possibly medical psychiatric treatment for the other associated conditions. There is no doubt, considering all of the medical reports, observations and testing, that Mrs. Smith is experiencing major stress and depression in combination with PTSD relative to the undiagnosed medical condition from which she is suffering. E. Mrs. Smith's statements during medical examinations and psychological testing have been reliable and consistent . Empirical medical and psychological data indicate that she was afflicted by a viral infection that doubtlessly affected her eyes and may have impacted her vestibular system, at least temporarily. She compensated by reducing her activity level, which exacerbated her sensitivity to head movements. The pain in her eyes remains to be explained medically. F. Psychiatric and psychological evaluations verify severe stress symptoms. This is exacerbated by postural changes (as verified by physiological data-EDR), emotional stress, and eye use. Medical symptoms have aggravated/exacerbated earlier underlying personality tendencies. G. The continuity of symptoms involving use of her eyes in combination with disequilibrium militates against employment, restricts her transportation capability and social activities and contributes towards daily headaches, anxiety and frustration. These factors certainly mount to cause a substantial detriment to the quality of her life. Consequently, Mrs. Smith is presently unemployable. Mrs. Smith has experienced--and continues to experience—emotional consequences due to the effects of this illness: loss of employment, inactivity, income and other enduring sequelae. These have directly and negatively impacted finances, family, socialization and self-esteem. Considering her personal career investment over many years, unless there is a radical improvement in her condition she may never again enjoy the same quality of life and sense of well being as prior to being driven into despair by the present illness.
|
|
Medical Disclaimer: This website is underwritten completely by Dr. Cooperstein.
The purpose of the content is to educate, inform and
recommend. Under no circumstances is it meant to replace the expert care and
advice of a qualified professional as rapid advances in medicine may cause
information to become outdated, invalid or subject to debate. Accuracy
cannot be guaranteed.
Dr. Cooperstein
assumes no responsibility for how information,
products and books presented are used and
does not warrant
or guarantee the content, accuracy or veracity of any linked sites. Dr.
Cooperstein makes no guarantee to any representations made by listings
in professionals or support services directories.
|